Male Infertility
Cause of Male Infertility
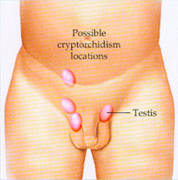
Cryptorchidism
Cryptorchidism

Cryptorchidism
Cryptorchidism
- Normal semen parameters are liquefaction in 30 minutes, volume 2-5 ml, pH 7.2 to 7.8, fructose present, sperm count ≥ 20 million/ml, sperm motility > 50% grade III, and > 50% sperm of normal morphology. If any of the parameters are abnormal, further evaluation is necessary.
- Usually a general examination does not reveal any abnormality. If the FEATURES ARE DYSMORPHIC, A KARYOTYPE IS OBTAINED. It may be 47, XXY (Klinefelter syndrome). If findings of general examination are normal, and karyotype is 46, XY, urologic examination is done. It may reveal the following abnormalities.
- VARICOCELE: there is varicosity of the pampiniform plexus. The diagnosis is unconfirmed by Doppler studies. It is treated by high ligation of spermatic vein (Palomo’soperation) or excision of the plexus.
- ATROPHIC TESTES: it may be developmental or acquired, as in bilateral mumps orchitis. The testes feel small. Exact volume of each testis is measuresd by an orchidometer. If a biopsy shows absence of seminiferous tubules and spermatogenesis, the treatment is artificial insemination with donor semen (AID) or adoption.
- CHRONIC EPIDIDYMITIS: broad spectrum antibiotics and an NSAID are given. If it is found to be tuberculous, it is treated appropriately.
- If the SEMEN VOLUME IS LOW (< 1.5 ML) and the man has abstained from coitus for the prescribed 5 days before the test, his urine is examined for sperm. Presence of sperm in semen suggests retrograde ejaculation. It may be due to extrophy of bladder, prostatectomy, resection of the bladder neck, diabetes mellitus, spinal cord trauma, sympathectomy, multiple sclerosis, urethral valves or strictures, or use of adrenergic blocking agents. If the condition persists despite adequate treatment of the cause, urine is alkalinized (NaHCO3 1 tsf PO q6h X 48 h), the man is asked to ejaculate while his bladder is empty, his uurine is then collected and centrifuged, and the sperm pellet is used for artificial insemination (AIH) after resuspension in Ham’s F-10.
In the absence of retrograde ejaculation, the man is treated with testosterone (T) if his sperm T level is low. If the volume remains low, a sperm concentration technique is used, and that sample is used for AIH.
- If other semen parameters are normal in presence of high volume (> 5 ml), no further treatment is required. If any parameters are abnormal, a sample is obtained for AIH by split ejaculate or swim-up technique.
- HIGH VISCOSITY is managed by sperm washing and intrauterine AIH.
- AGGLUTINATION OF SPERMATOZOA may be due to antisperm antibodies, which are detected by immunological tests. Treatment with glucocorticoids is not very satisfactory. Sperm washing and AIH appears to be promising.
- PRESENCE OF PUS SELLS is due to infection of accessory glands. Appropriate antibiotic is given after microbiologic studies.
- IF FRUCTOSE IS ABSENT, the vasa deferentia are palpated. If they are found to be absent, a sample for AIH or in vitro fertilization (IVF) is obtained by epididymal aspiration.
- If there is AZOOSPERMIA, or all parameters are abnormal, including oligozoospermia (sperm count < 20 million/ml), asthenozoospermia (sperm motility < 50%, < grade III), necrozoospermia (dead sperm > 50%), teratozoospermia (abnormal sperm > 50%), sperm FSH, LH, and T levels are estimated.
- IF HORMONE LEVELS ARE NORMAL, TESTICULAR BIOPSY is done. If spermatogenesis is arrested or absent, adoption or AID is advised. If it is normal, vasography is done. Obstruction in a vas is treated by microsurgical reversal of the obstruction. Absence of vasa is managed by aspiration of a spermatocele and the sample is used for AIH of IVF.
- HIGH LEVELS OF FSH, LH AND LOW LEVEL OF T INDICATE TESTICULAR FAILURE. The treatment is adoption or artificial insemination with donor semen (AID).
- HIGH LEVEL OF FSH AND NORMAL LEVELS OF LH AND T ARE DUE TO ISOLATED GERMINAL CELL FAILURE. If there is oligozoospermia, the treatment is AIH or IVF, depending on the count. If there is azoospermia, the treatment is adoption or AID.
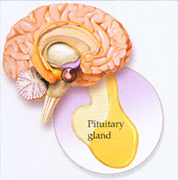
- Low levels of FHS, LH, and T are evaluated by serum prolactin (PRL) assay and CT scan of head. If both are normal, the condition is idiopathic. It is treated by human menopausal gonadotropin. High PRL level and normal CT scan are treated with bromergocriptine, repeating the CT scan after 6 months for a pituitary microadenoma. If a pituitary tumor is found (high PRL level, tumor in sella turcica), the patient is referred to a neurosurgeon for treatment.
- NORMAL FSH AND HIGH LH AND T LEVELS ARE DUE TO ANDROGEN INSENSITIVITY. The treatment is adoption or AID.
- Empiric forms of treatment are as follows:
- Stimulation: clomiphene, tamoxifen, hMG / hCG, testosterone, mesterolone, testolactone.
- Antioxidative therapy: vitamin E
- Mast cell blockage: ketotifen
- Immunomodulatory therapy: zinc
- Improving microcirculation: pentoxifylline
- Rebound therapy: testosterone



